
Check out the new page on http://www.drbenjamino.com
elbow dysplasia
Frankie’s Journey: Part 2

After the diagnostics were performed (reviewed in the previous segment), a decision needed to be made as to which issue was to be addressed first. This is often a tough decision and must be made with the experience of your trusted veterinarian. My criteria consisted of which leg was most affected and the fact that I had already decided to address his hips with a total hip replacement. In my opinion (and supported clinically), a total hip replacement was a better option than other procedures available for canine hip dysplasia. Certain growth plates (centers of bone growth) need to be closed prior to performing a total hip replacement making the minimum age being around 10 months of age. This made our decision easier and the decision to address the elbows was made.
Surgery for his elbows was staged; the left elbow surgery performed on December 6, 2013 and the right elbow addressed on February 14, 2014 (Happy Valentine’s Day!). The time period in between was used for physical therapy and maximizing the results of the surgeries. Identical surgeries were performed on both elbows due to the similarity of the disease process occurring. An elbow arthroscopy was performed, which revealed the cartilage flap (osteochondritis dissecans (OCD)) and a fragmented coronoid process (FCP) The OCD flap was removed and the FCP segment was removed. The damaged bone under the OCD flap was removed with a shaver until healthy bone was present. Since the diseased area of the elbow was on the inside (medial) aspect a specialized procedure to displace weight to the central and outside (lateral) aspects was performed. This procedure is called a sliding humeral osteotomy (SHO). This procedure is fairly aggressive and involves a bone cut in the middle of the humerus bone and a plate/screws placed.
Below are images of the elbow arthroscopy showing both the OCD lesion and the FCP segment.

Noted the line in the cartilage outline a fragmented coronoid Process (FCP).

Note the underlying bone (pink). This is usually covered by cartilage, however the cartilage has become a flap.
Following the elbow arthroscopy, the SHO procedure was performed. Below is a radiograph of the procedure.

Note the cut in the middle of the humerus and the shifting of the bone.
Frankie’s Journey

I want to share this story of Frankie with everyone, as it will be an ongoing story for the next year or so as we continue to help him though this hard time. Frankie was seen by me about two months ago when he was six months old. He is a Golden Retriever that presented for lameness in all legs. He had been enrolled in a service dog program when his owners started to realize that he was having trouble walking. He was referred to me after being evaluated by a local neurologist, who couldn’t diagnose a neurologic issue.
On presentation, Frankie had lameness (limping) in all four limbs. He had pain on manipulation of both elbows, especially when pressure was placed on the inside of the elbows. He had a shortened stride to both hind limbs and was painful on hyperflexion and hyperextension of both hips. Another interesting finding, was that both hips could be felt subluxating on exam (positive ortolani test). This means that you could feel the femoral head rub and partially come out of joint.
Radiographs (x-rays) were taken of all joints and a diagnosis of bilateral elbow dysplasia (osteochondrosis dissecans (OCD) and fragmented coronoid process) and bilateral hip dysplasia was made. Unfortunately, Frankie’s career as a service dogs had to abruptly end. Because of the extensive orthopedic work that would be needed (both elbows and both hips) he was in need of a new home to care for his special needs. My wife and I may be a glutton for punishment, but we thought long and hard about this decision and decided to open our home and give this Golden puppy a second chance.
So my intention for this “Featured Article” segment is to follow the course of Frankie’s treatment including surgery, recovery, physical therapy, and final outcome. I feel that other owners may be in similar circumstances and this may help encourage some and educate others. This will also give a forum to discuss congenital issues such as elbow dysplasia and hip dysplasia. Going through these issues on our own pet, has been an eye-opening experience for us and me professionally. I can now relate to my patients and clients on a much more personal level.
In future segments (soon to follow) we will go through diagnosis, diagnostic test (radiographs and CT scan) and surgeries. So far, Frankie has had surgery on one elbow and is recovering well from that, we will go into more specifics as we go. The plan will be for the other elbow in the near future and then total hip replacements.
Also, please do not ask to donate financially to Frankie, I am not trying to raise money. I am just trying to educate others. There are so many generous people out there and there are many charitable animal organizations that can benefit from your generosity, as it is always appreciated!

Elbow Dysplasia
What is Elbow Dysplasia?
Elbow dysplasia is a multifaceted disease that can affect both juvenile and mature dogs. The complex of elbow dysplasia can be divided into the following categories:
– Fragmented coronoid process (FCP)
– Medial compartment disease (MCD)
– Osteocondrosis dissecans (OCD)
– Ununited anconeal process (UAP)
– Elbow incongruency (EI)
– Ununited medial humeral epicondyle
One or more of these problems can be affecting your pet and can cause a varying amount of lameness. We generally believe that elbow dysplasia is a congenital issue and affects mostly larger breed dogs, but can affect small breed dogs, as well.
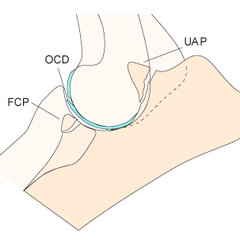
Diagram of the canine elbow.
The “ins” and “outs” of Elbow Dysplasia
Clinical signs: The most common clinical sign that is reported in dogs is front leg lameness. This can vary in intensity and can come on slowly or acutely (all of a sudden). Some pets will develop swelling at the elbow. Typically, limping becomes worse with activity and can subside with rest. Unfortunately, clinical signs can vary from pet to pet.
Diagnosis: A thorough exam is recommended to isolate the elbow as the problem. It is important to evaluate the whole front leg as well as the opposite leg for any abnormalities. Because elbow dysplasia is congenital, both elbows tend to be affected (>80%).
Radiographs – In juvenile dogs, changes can be very minimal. Classic radiographic signs include: osteoarthritis (anconeal ridge is an early sign), sclerosis (thickening) of the ulna, joint swelling and fragmentation of the medial coronoid process (33-50% visible on x-rays). OCD and UAP lesions typically will be evident on x-rays. It is standard to take three views of each elbow.

Patient with elbow dysplasia. Note the osteoarthritis present.

Patient with an ununited coronoid process.
CT scan – Computed tomography (CT scan) may be necessary in some cases to make a diagnosis. A CT scan is a different type of x-ray and requires that your pet be anesthetized. The advantage of a CT scan is that it gives us a greater detailed image of the joint allowing us to detect mild changes. Sensitivity of a CT scan is >90% in diagnosing elbow dysplasia.
3-D image reconstruction of an elbow CT scan.
Treatment: Successful treatment of elbow dysplasia can occur with early diagnosis and treatment. The more advanced the arthritic changes (which will occur with time), the less successful treatment becomes. The following is a brief overview of the current treatments that are performed, usually in combination.
Arthroscopy – Considered to be the “gold standard”, arthroscopy allows us to obtain critical information about the joint by looking in the joint via a minimally invasive approach. A scope and camera are introduced into the joint and the joint surfaces are assessed for arthritis, cartilage wear, incongruency and fragments. If fragments exist, these can be removed with arthroscopy. If substantial cartilage wear is present other procedures may be recommended.
Conservative management – this includes non-steroidal anti-inflammatories drugs (NSAIDs), supplements, physical therapy, acupuncture, and regenerative stem cell therapy. Unless your pet is very severely affected this therapy is often used in conjunction with arthroscopy and surgical management.
Advanced surgical procedures – Depending on the assessment of the joint, other procedures may be recommended such as the following: sliding humeral osteotomy (SHO) or unicompartment elbow replacement (CUE) for medial compartment disease, biceps tendon release and elbow replacement surgeries.
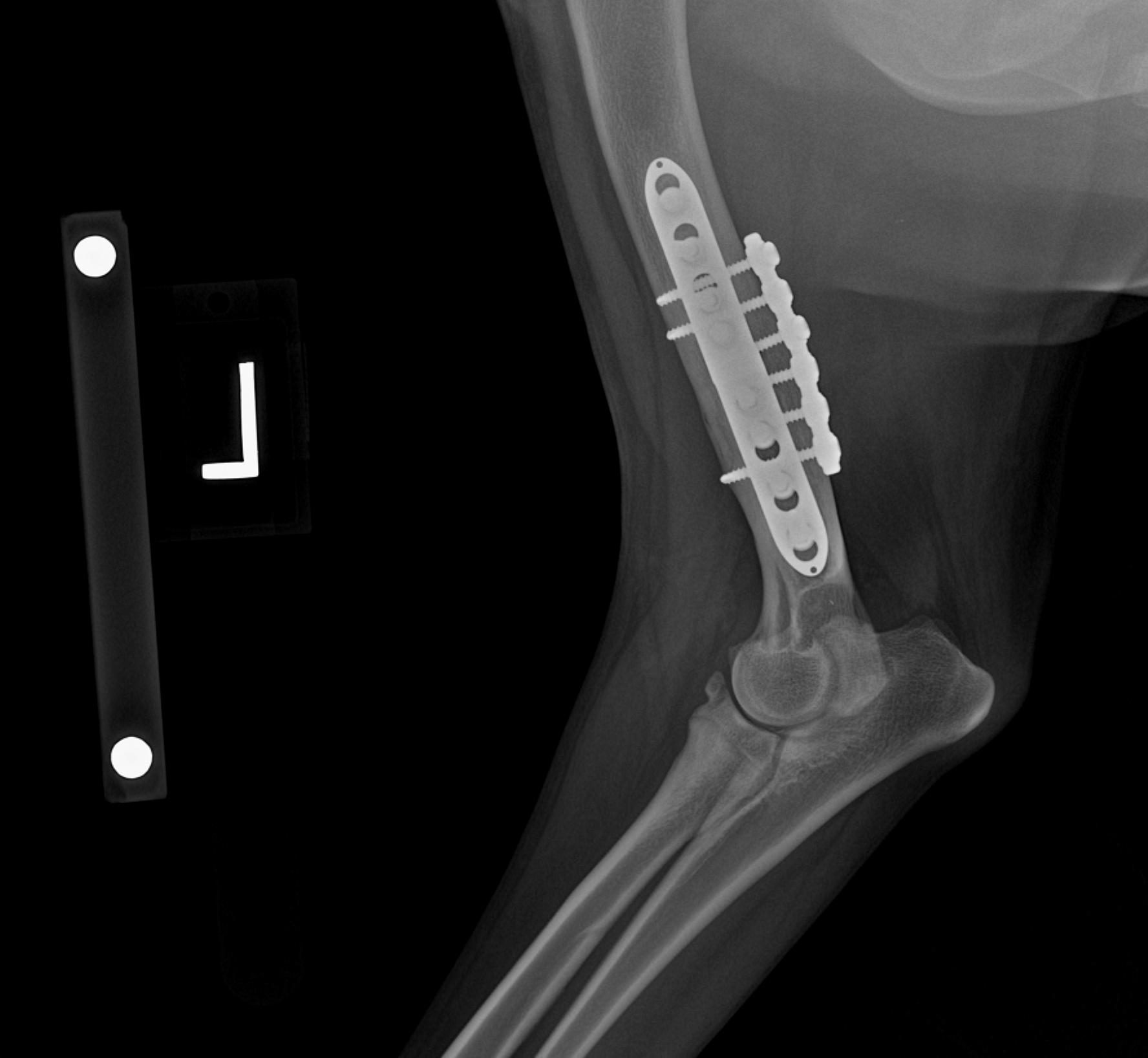
Patient with a Sliding Humeral Osteotomy (SHO).
“Will my dog get better?
Prognosis – With early diagnosis and aggressive treatment, the success rate of the treating elbow dysplasia is ~80%. This generally entails elbow arthroscopy and sometimes more advanced procedures. Also, if changes are detected on the opposite leg, arthroscopy of this leg is recommended as well. In about 20% of the cases we need to combine multiple treatments and sometimes arthritis and discomfort will still progress.
Elbow replacement surgeries are still up and coming and can be considered in pets with “end-stage” changes to the elbow.
