
TO VIEW THE VIDEO OF THE STICK REMOVAL, PLEASE VISIT THE FACEBOOK PAGE: Kevin Benjamino DVM, DACVS and like the page while you are at it!!
This case certainly deserves to be designated as a case of the month! I have uploaded some images and video. As for the video, as a fair warning, it may not be suitable for children due to the surgical images.
Luke is a 2 1/2 year old American Staffordshire Terrier who presented to the surgery service at Affiliated Veterinary Specialists (Orange Park) for evaluation of a non-healing wound over his left side, near his last rib. The owners and family veterinarian had been managing the non-healing wound for the past 6 months with different antibiotics and even had a surgery to try and identify a reason or source of the the wound. Outside of the non-healing wound, Luke was a very active dog and nothing could slow him down. the rest of his physical exam (other than the wound) was normal.
Part of Luke’s history is that he is a wild boy and loved to chase sticks and run through the woods, etc. One of the top reasons why some dogs develop non-healing wounds is due to foreign material that can migrate or move around the body to different areas. Some dogs are responsive to antibiotics which keep secondary infections controlled, however once the antibiotic is stopped, the wound comes back (which is what has happened with Luke). This had us suspicious that we could be dealing with foreign material that could be the cause for Luke’s signs. Other causes for a non-healing wound would be resistant infections and/or fungal infection, cancer, etc.
The next step for Luke was to perform some basic diagnostics including some radiographs (x-rays) of both his thorax (chest) and abdomen to rule out anything obvious or a communication from the outside into these body cavities. The x-rays were relatively unremarkable. With Luke under anesthesia just prior to surgery, a contrast study called a fistulogram was performed. A foley catheter was introduced into the non-healing wound and contrast fluid was injected. This fluid will show up white on x-rays. On this test, we were able to see some uptake of the contrast around an object in between the 11th and 12th rib. This test was very useful in showing us where we needed to focus our attention surgically.
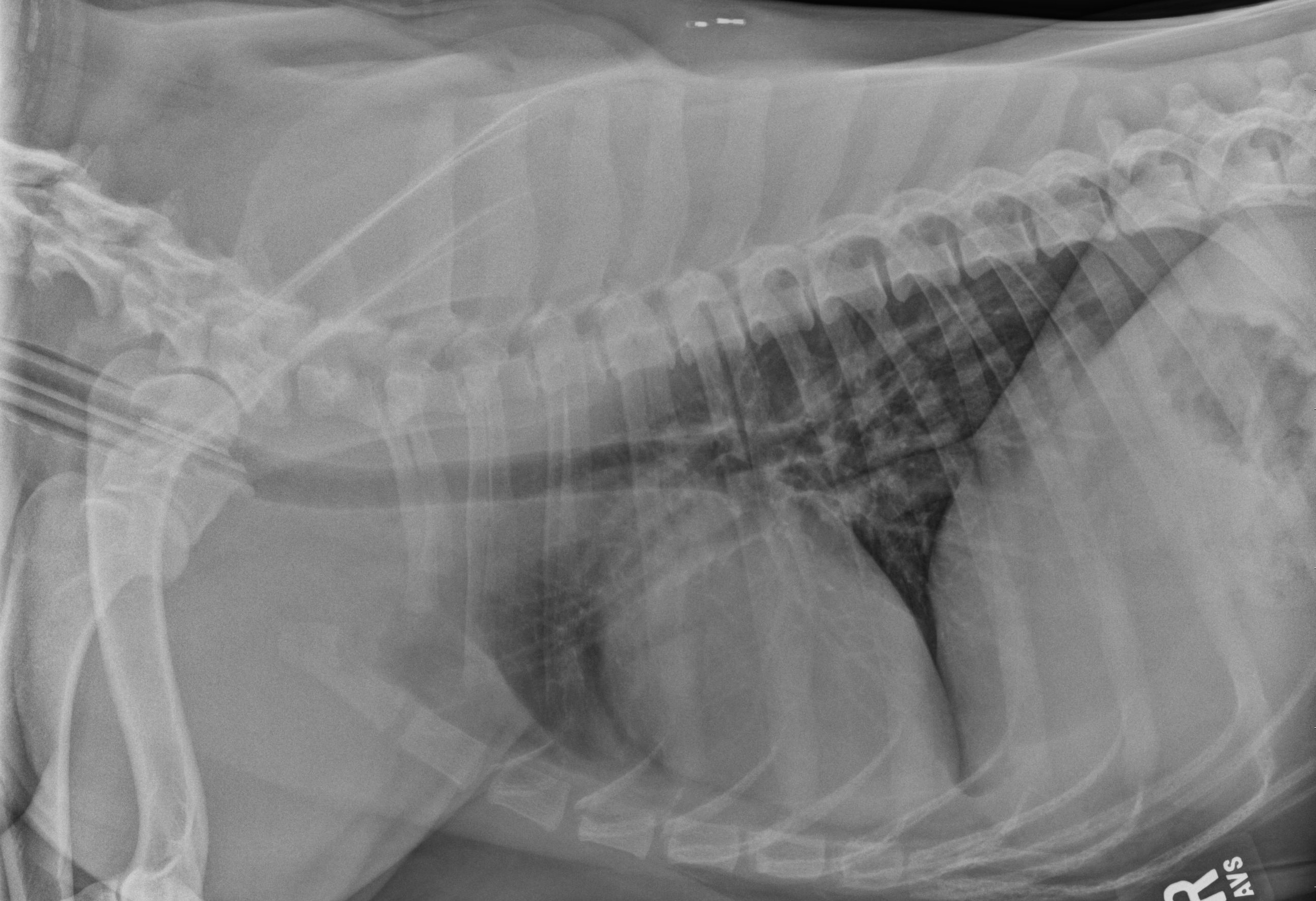
Plain chest radiograph (x-ray)

Plain abdominal x-ray.
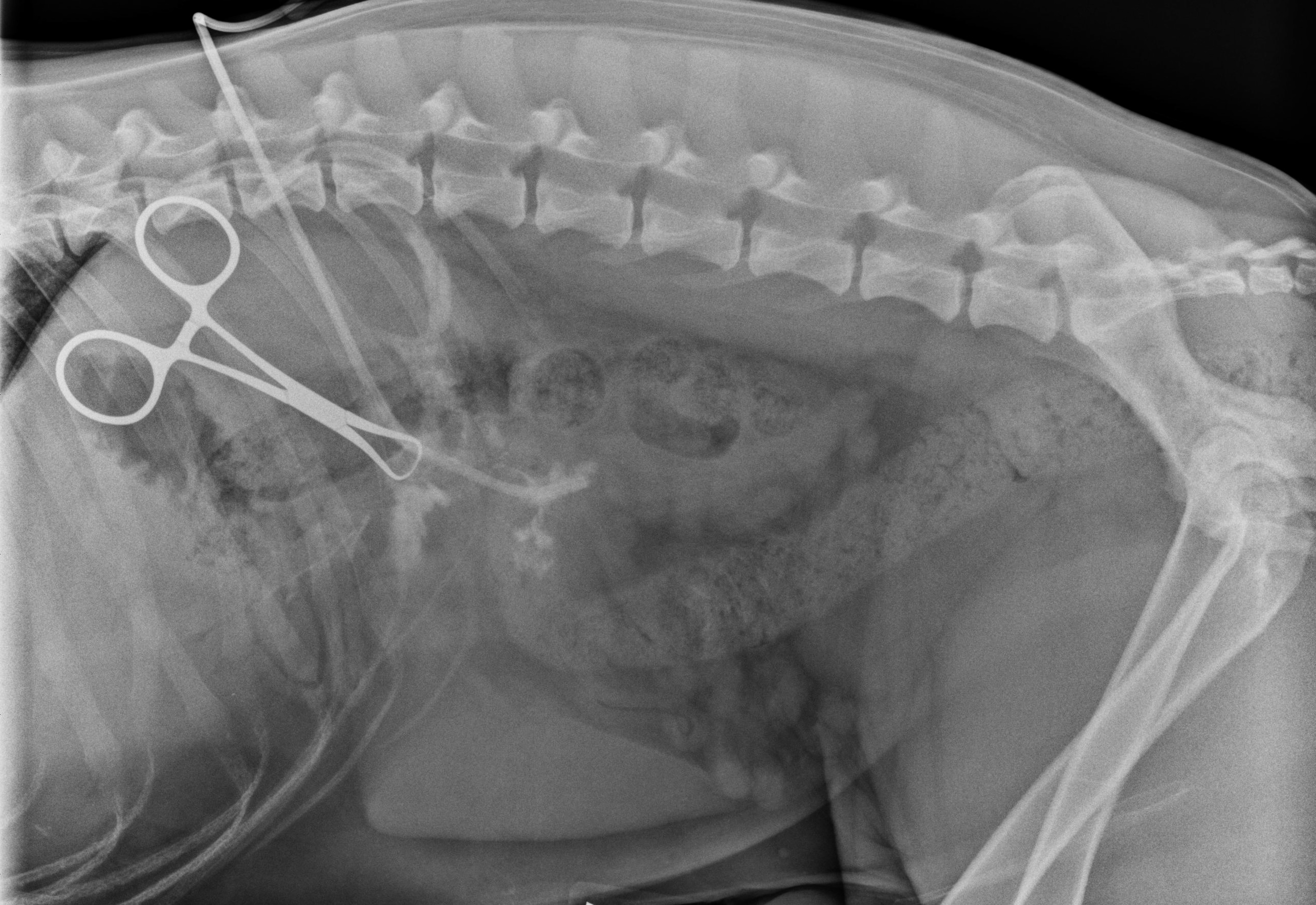
Fistulogram image: Notice in front of the clamp there are small white lines outlining the stick.
The video pretty much says it all! On dissection in between the 11th and 12th rib (deep to the rib) we found a stick that was lodged there and it was successfully removed. This was a very gratifying surgery. You may be asking, were was the stick – which is an excellent question, did it come from the abdomen, chest, etc? If there was direct communication within the abdomen, then we would be concerned with a septic (infection) peritonitis and likewise if it were within the chest cavity we would be concerned with a pyothorax (infection in the chest cavity). To help us determine this, another foley catheter was introduced (after copious flushing) into the space that was occupied by the stick and everything else was closed around the catheter. Contrast was injected into the catheter and a x-ray taken which showed the contrast in the stomach and not in the body cavity. Sequential x-rays were taken which showed the contrast in the gastrointestinal tract and not outside.
Amazingly, I believe Luke had swallowed the stick at some point (longer than 6 months ago) and the stick had migrated from the stomach wall to the body wall. Most likely the stomach had been tacked or pinned to the body wall creating what is called a stoma, sealing the stomach to the body wall. Luke is quite a remarkable dog for withstanding this condition. On multiple rechecks since surgery, he has been doing very well – like nothing every happened. He is one for the record books!!!
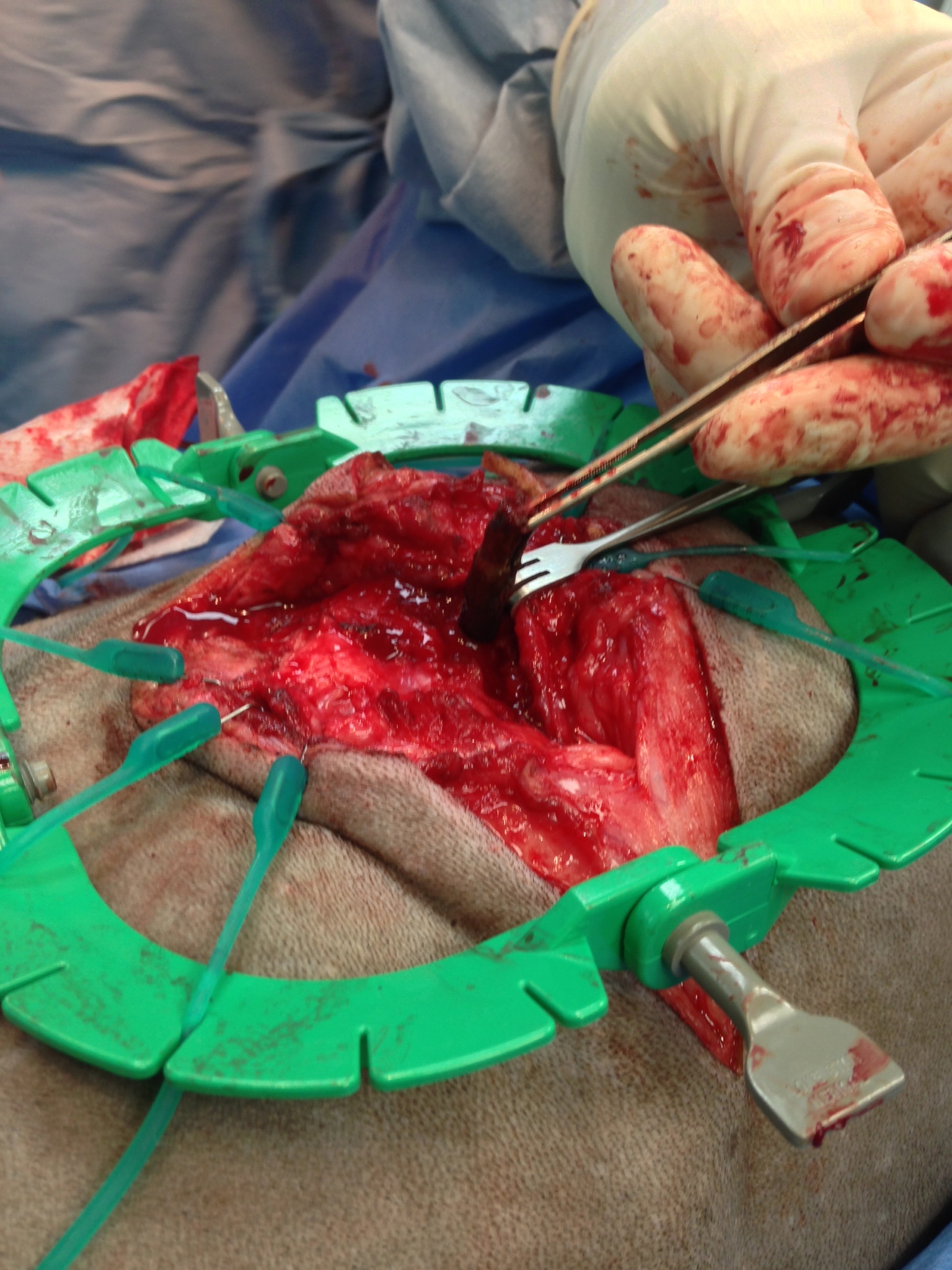
Here is the stick as it is lodged under the rib.

Here is the stick after it was removed from Luke
