
Bone fractures in pets are a relatively common occurrence in veterinary medicine. Injuries to pets can occur many ways, with the most common being vehicular trauma (hit by car). This brief article is meant to inform owners that not all fractures should be managed the same way and that as fracture repair advances in the human orthopedic field so are the advances in the veterinary field. No longer do we need to rely on pins, wire, and a prayer. The advanced surgical techniques can be thanked due to our increasing appreciation of biomechanics and the different forces on various areas of the body. Many times I have been asked “can you cast that fracture?” The answer to the question is “sometimes”, however most fractures encountered have a much higher chance of healing with some sort of surgical fixation (internal or external). I always remind owners that with our canine or feline patients, they will be trying to use the fractured limb much sooner than we would, which means more pressure on our support. Also, be reminded that when we have a forearm (or upper arm) fracture we won’t be required to walk on it like our pet counterparts.
Our first goal with fracture fixation is how can we make this fracture stable immediately, that will last through the healing process. To do this the surgeon must have a full understanding of biomechanics to appreciate the different forces on the bone (tension, compression, etc). There is no such thing as “cookie-cutter” fracture repair. While many fractures are similar, none are exactly the same. Some may be comminuted (multiple pieces), develop fissures (splits down the long axis of the bone), exposure to the outside (open, contaminated), and be intra-articular (enter into the joint) and require special consideration. It is rare, in the day with veterinary specialists that limbs need to be amputated due to the fracture – the more common reason for amputation would be due to severe neurologic impairment (no feeling, etc). Other goals with fracture fixation include: how do we minimize trauma to soft tissue (skin,muscle, etc), minimize bleeding, minimize infection risk, and maintain blood flow and clots that initially develop around the fracture site that aid in quicker healing.
Fracture repair has evolved over the years from full exposure and full reconstruction of the bone (even with multiple fragments) to minimal reconstruction biological osteosynthesis) and soft tissue disruption (Minimally Invasive Plate Osteosynthesis (MIPO)). This articles goal is to introduce the reader to some of the newer technologies available to the veterinary surgeon and your pet. These techniques are aimed at early recovery and return to function of your pet. I would be remiss if I didn’t mention that exercise/crate restriction is needed during the post-operative phase and can be 8-12 weeks in duration, depending on the type of fracture and age of pet. Please follow the advice of your veterinarian.
Early plates that are still used today (and many times the appropriate choice) are called Dynamic Compression Plates (DCP) or Limited Contact – Dynamic Compression Plates (LC-DCP). There are many cases where this is either the most appropriate option or the only option. The plate must be placed flush against the bone after the bone is reconstructed or supported. Screws go through the plate into the bone through pre-drilled holes. Remember wood-working concepts, as the threaded holes in the bone accept the advancing screw, the screw starts to bring the bone to the plate as you tighten the screw. This bone-to-plate interface (touching/squeezing) is where this type of repair gets it strength. If there is no bone to plate contact, this becomes a very weak fixation. This also demands that the plate is precisely contoured to the bone before application. Some downsides to this fixation is that the fracture must be fully exposed and manipulated (delayed healing, increased risk of infection, soft tissue trauma to an already traumatized area) and that if not perfectly pre-contoured it could weaken the repair or offset the fracture alignment to a degree. There are advantages to this type of fracture repair as well, such as allowing the bone to accept some of the weight bearing load (if a two piece fracture), being able to compress the fracture ends and being able to compress fissures and fragments through the use of screws placed in “lag” (compression) fashion. So there is definitely a place for this type of fixation and in appropriate cases can be the best option.
DCP plate used to stabilize a radius fracture.
Early fracture fixation that tried to minimize soft tissue trauma while providing a strong fixation was the external skeletal fixator (ESF) which encompasses both linear and circular external fixation. These allow the surgeon to place pins of varying sizes in the bone, where the ends remain outside of the limb and connect to a bar or ring for support. Case selection is key as with any type of repair and they certainly have their place in fracture fixation. Surgeon experience and knowledge of repair mechanics is necessary. Some ideal cases may be (but not limited to): some juvenile fractures, open (infected) fractures, intra-articular (or near joint) fractures, etc. The benefit of this fixation is that once the bone is healed, all the implants are removed. Also, sequential removal of pins can be performed to destabilize the repair – which can be beneficial in fractures that are delayed in healing.

A linear external fixator used to stabilize a tibial fracture.

An external fixator used to stabilize a tibial fracture
More recent repair options are locking plates. Many companies have began production of locking plates and this article is not meant to show favoritism to any company. The basic concept with this technology is that the screws used actually lock into the plate to provide more stabilization. Previous designs (see above) depended on the bone to plate interface. Locking plates are dependent on the strength of the screw to plate interface, which is typically much stronger. Screws “lock” into the plates by either a conical locking mechanism (Morse taper phenomenon – for all the engineers in the audience) or by threading into the plate (threads on the screw heads match the threads in the plate holes). Many hours of mechanical testing has gone into these types of plates both on the human and veterinary side and have proven their strength. A benefit of this increased strength is the need for less screws than in the earlier described plate designs. We can achieve our desired strength of fracture repair with less implants (less can be more with regards to fracture fixation). Another big benefit is that we no longer are so concerned about contouring the plate to the bone , which allows us to not touch the fracture site to aid and facilitate healing. Remember standard plates bring the bone to the plate as the screw tightens, with the locking plate design, as the screw contacts the plate and locks the bone stays stationary. This design also allows us to perform MIPO techniques with a strong fracture fixation. By in large, this type of fracture fixation is leading the way in both human and veterinary surgery. The downside is that these plating systems are usually only available at veterinary surgical centers, but again they offer a great advantage to fracture management.


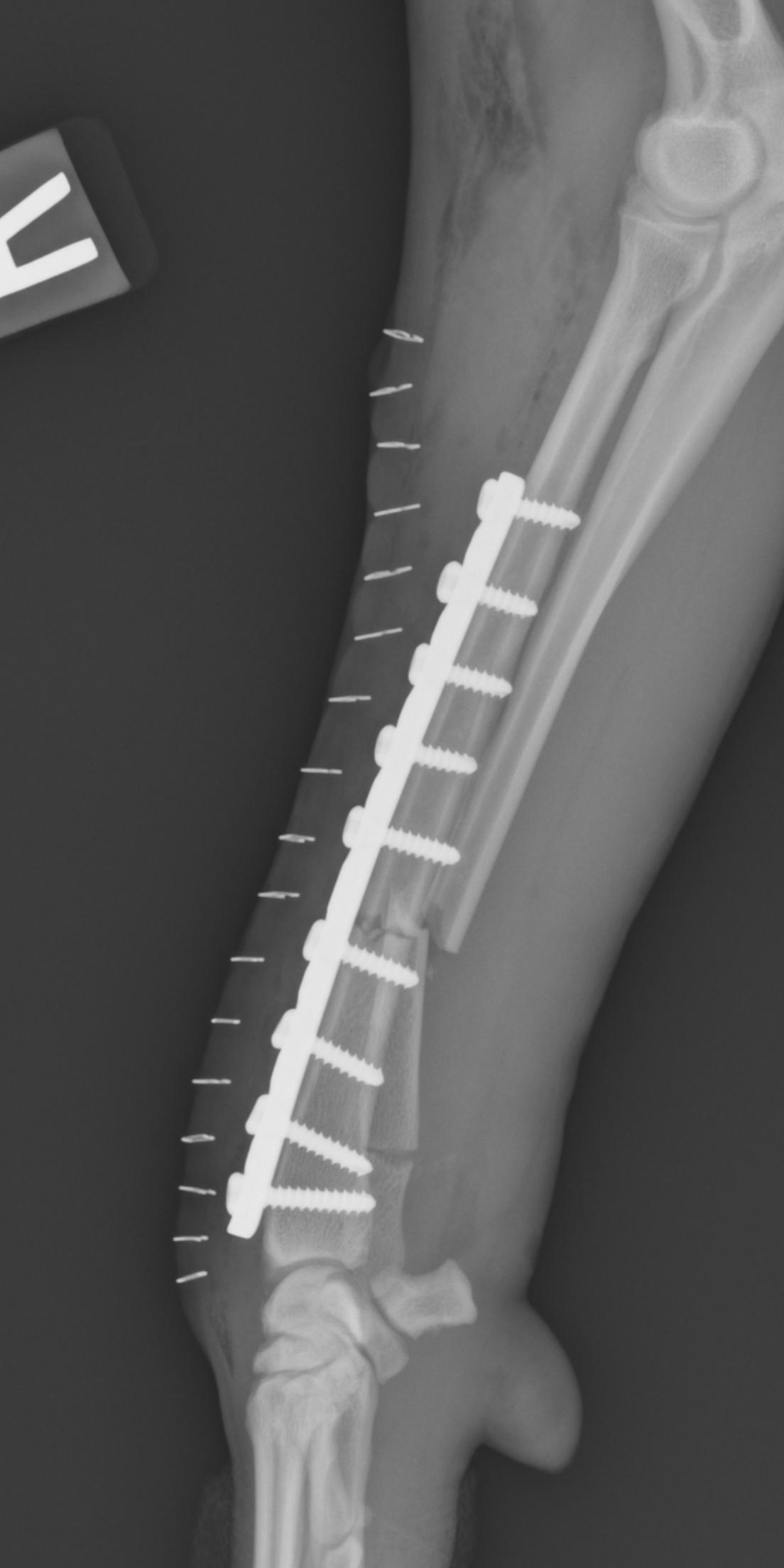
Fracture repaired using a minimally invasive (MIPO) technique and locking plate.

Fracture repaired using a minimally invasive (MIPO) technique and locking plate.
Again, when deciding what type of fracture fixation is best there are many factors to consider and that decision would be made best by your veterinary surgeon. Also, not all types of fixation have been mentioned in the article. We are very fortunate to be living in this time where veterinary medicine is advancing so we can provide greater benefit for our best friend and loyal family members.
– Kevin Benjamino DVM, DACVS





