
Check out the new page on http://www.drbenjamino.com
dog knee
October 2013 Case of the Month
October Case of the Month

Scooter (left) enjoying the beach!!
For October’s Case of the Month, I have selected a relatively common problem that we see in veterinary medicine – cranial cruciate ligament ruptures. Cranial cruciate ligament (CrCL) ruptures (more commonly referred to as an ACL tear after the human literature) are commonly seen in the practice of veterinary surgery, in fact they are our most common orthopedic case that we see. This disorder affects both the large and small dog, from the Great Dane to the Chihuahua and can affect dogs of any age most commonly the middle age dog. If you would like further details about this specific disorder, please see the previous posts regarding cranial cruciate ligament ruptures (click on the orthopedics tab in the menu bar).
Scooter is a 5 yr old Labrador Retriever that presented for lameness in both hind limbs. His history was such that he was lame in the left hind limb about a year ago and had a previous surgical procedure to address the CrCL performed, to which he responded well early on but became increasingly lame again in the leg and then developed a right hind limb lameness in addition. The procedure previously performed on the left stifle (knee) was not documented and no radiographic implants were used in or around the stifle. Also, Scooter has a chronic history of hip dysplasia and osteoarthritis in both hips to compound his issues.
Physical Exam:
Scooter could walk with assistance, however really struggled in both hind limbs to ambulate. Also, you could see Scooter shifting his weight to his front legs, which is a very classic feature for dogs with CrCL ruptures that affects both stifles. Our physical exam revealed that both (left and right) CrCL were ruptured and we highly suspected bilateral meniscal injuries/tears. While some discomfort could be elicited from manipulation of his hips, the majority of his discomfort and inability to walk was from his CrCL ruptures and meniscal tears.

Right knee – note the joint swelling, arthritic changes, and forward movement of the tibia in relation to the femur.

Left knee – note the joint swelling, arthritic changes, and forward movement of the tibia in relation to the femur.

VD pelvis x-ray – note the chronic signs associated with hip dysplasia.
Surgery:
Surgery was scheduled soon after his initial exam, all his pre-operative work-up was otherwise normal. Most of the time we try to stage each leg. The big reason for separating out surgery on each leg is to reduce the risk of complications such as infection and implant breakdown. Some cases, like Scooter, we chose to do both especially if they are severely affected on both legs like Scooter.
At surgery, bilateral cranial cruciate ligament ruptures were noted, along with bilateral medial meniscal tears. All those findings can be very painful for the patient. Both meniscal tears were debrided (removed) and bilateral tibial plateau leveling osteotomies (TPLOs) were performed. For more detailed information about ways we correct CrCL tears, please view that page on this website.

Right knee – following TPLO surgery.
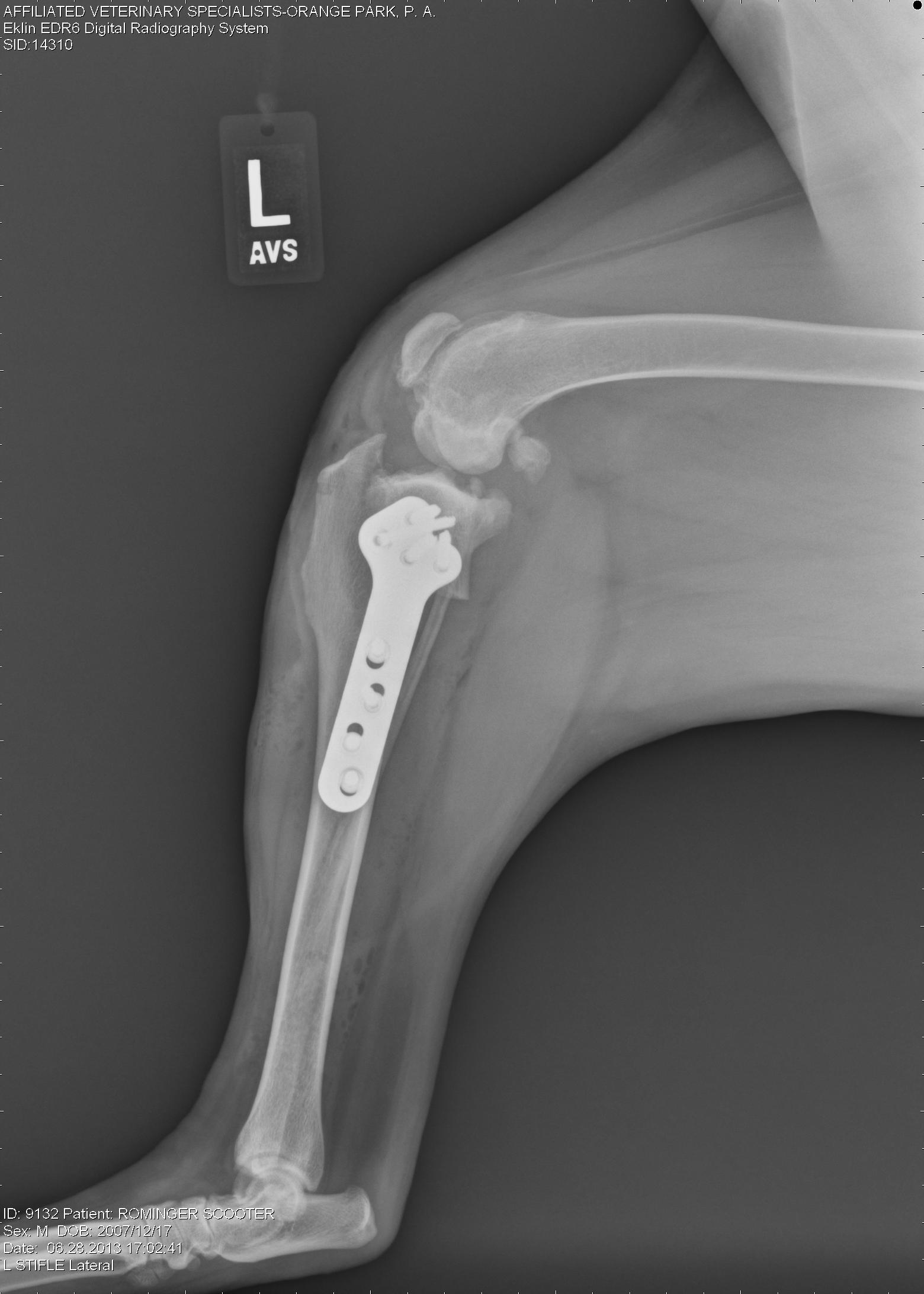
Left knee – Following TPLO surgery.
Post-operative care:
As you can image, we treat these patients very carefully. In human medicine, physical therapy and rehabilitation is started almost immediately following surgery. As soon as a patient leaves the operating room, we start icing of the surgical site. That is followed but passive range of motion exercises and short, assisted walks and frequent icing after sessions during the first two weeks. A fairly strict physical therapy program is given to owners and in some cases, organized physical therapy sessions are scheduled under the supervision of a certified canine rehabilitation therapist (CCRT). I generally tell the owners that their commitment to physical therapy is as important as the surgery performed. In Scooter’s case, his owners were very dedicated to the whole process and 16 weeks later he is back to doing his normal activity, which includes running, swimming, and of course lounging around from time to time.

Swimming at dusk.

Happy dog basking in the sun!!

Scooter and his buddy enjoying a swim!!
Happy Holidays
I want to take a moment to thank everyone for their continued interest and support of this blog. Your continued support has meant a lot to me and allowed me to continue to post various topics. I want to wish everyone Happy Holidays during this joyous time of the year! I wish you all the best in the New Year too! Keep your pets safe throughout this time, but definitely spoil them (we want them to ring in the New Years without any ailments)! Please continue to follow this blog!
Seasons Greetings!!
Kevin
Minimally Invasive Surgery – Laparoscopy

View of the liver and diaphragm laparoscopically

- View of the right ovary during a standard laparoscopic spay.

- Abdominal view of a laparoscopic gastropexy.


What is laparoscopy? This is an advanced surgical technique that utilizes cameras and instruments that are introduced into the abdomen via small incisions (portals). This type of surgical procedure is becoming more and more common in human medicine. It is not uncommon to hear about gallbladder removals, “lap band” procedures and many other operations being performed this way. It is really becoming the standard of care – so why not for our pets? Certainly the technology is there! The more and more we get comfortable with these techniques, the more we will be able to do.
The basic concept of laparoscopy is to make portals that allow the introduction of a camera and instruments. The actual surgical work is done within the abdomen by visualizing it on a video monitor. Before attempting laparoscopic surgeries, the surgeon needs to be comfortable with performing the surgery in an open approach, because there are times, when laparoscopy is not the best approach and the surgery needs to be converted.
What are the benefits of laparoscopy? The most notable benefits are patient comfort, soft tissue damage (termed morbidity), excellent visualization (images are magnified), shorter hospital stays. All these combined form a convincing argument for laparoscopic surgery.
One of the most common procedures performed is the ovariohysterectomy (spay). This can be performed from 0.5 cm and 1.0 cm incisions. This is a very quick procedure and allows the surgeon complete access and visualization of the ovaries and uterus. Specialized sealing devices allow the surgeon to remove the full uterus and ovaries with minimal bleeding and incisions. Another benefit is that with the small size of the incisions, there is low risk of herniation of abdominal contents, and the patient can return to activity in about a week.
The spay is many times combined with a prophylactic gastropexy in the larger breed dogs. This is a procedure that allows the stomach to be attached to the body wall to prevent deadly twisting of the stomach. This is a very effective procedure. For more information, please visit the previous blogs entitled GDV.
Other more complex procedures include multiple biopsies, adrenalectomy, gallbladder removal, liver mass resection, cryptorchid testicle removal, etc. As more experience is gained with laparoscopy the more we can do. If you have questions about laparoscopy feel free to comment or ask your veterinarian and veterinary surgeon.
Minimally Invasive Surgery – 1
I hope everyone is having a great weekend! The next series of topics is join got focus on minimally invasive procedures. This is of particular interest of mine. There are multiple implications of this terms, I am going to focus on laparascopy, thoracoscopy and arthroscopy.
As medicine advances in both the human and veterinary world, we are starting to do more with less. What I mean is that through smaller incisions and better technology we address more and more surgical problems. The benefit of this is shorter hospital stays, decreased complication rte, decreased infection rates, and decreased soft tissue trauma and post-surgical pain. We are very lucky to have all this new technology available to us.
Here is a definition of the terms:
Laparascopy: Abdominal surgery being performed with a scope/camera via a small portal incision. Multiple other portals are made to introduce instruments. All procedures are performed within the abdominal cavity. Laparoscopic-assisted means that part of the procedure is done with cameras within the body cavity and part is done via small incisions outside of the abdomen.
Thoracoscopy: Same definition as above, however this pertains to the chest or thorax. This is a very useful modality and is used to treat various cardiac, pulmonary (lung) and esophageal problems.
Arthroscopy: Same definition as above, however this is performed on the joints. This is a very common use in veterinary medicine and is thought to be the gold standard in joint evaluation. The most common joints evaluated through this are the elbows, shoulders and knees, however the wrists (carpi), ankles (hocks/tarsi), and hips can be evaluated. Just think, if you have an ACL injury, it is very common for you to have your knee scoped, why not your best friend?
ACL Injuries in dogs – treatment
This topic is usually approached cautiously. I will list the most commonly performed procedures for stifle (knee) stabilization. As a surgeon I recommend surgical management for ACL tears in the dog. If no surgery is performed the body will typically develop enough scar/fibrous tissue to stabilize the knee, however the timimg of this is very variable and the secondary arthritis can be severe in some cases. Surgical stabilization will create a stable joint at the time of surgery.
Direct replacement of the ACL has been attempted, but as of this time, has not been very successful. As I mentioned before, I will perform an arthroscopy (minimally invasive) and look in the joint with a small camera. This allows me to assess the ACL, debride the remnants of the ligament, and evaluate the rest of the joint especially the meniscus. If the meniscus is damaged this can also be addressed arthroscopically.
Common knee stabilization procedures:
1. Tibial Plateau Leveling Osteotomy (TPLO) – This procedure is a very common procedure that addresses the tibial plateau angle (TPA) or incline/slope of the tibia (refer to previous blog). With this procedure a circular cut is made under the joint in the tibia. Based on a calculation the top of the tibia is rotated to make the top of the tibia relatively flat. This relieves the tension and forward directed force from the ruptured TPLO. This is done in both partial or complete tears to the ACL. After the top of the tibia is rotated a plate and screws are placed on and in the bone. This is a widely used procedure that is typically very successful in returning the patient to near normal function.
2. Tibial Tuberosity Advancement (TTA) – This procedure is also a “bone-cutting” procedure but the osteotomy is not directly under the joint. It is in an area called the tibial tuberosity and is directed vertically (see picture). The idea is to alter the angle that the patellar ligament inserts on the tibial tuberosity to alter the amount of force the quadriceps exert on the stifle and eleviate the forward motion of the tibia. This also, is a successful procedure for stabilization of the knee joint for the partial and complete ACL tear.
3. Extracapsular stabilization – There are many variations of this technique whcih are beyond the scope of this blog. The general idea is to use a prosthetic ligament outside the joint running from the back part of the femur to the front part of the tibia to stabilize the knee joint. This can be a very successful procedure in the small breed dog, but looses its consistency (of being successful) in the larger, more active dogs. Also, we tend to see continuation of arthritis when compared to the TPLO and TTA.
As a surgeon, I try to guide the owner to a decision that will be the best fit for the patient based on many variables. The procedure that I perform the most is the TPLO, however, I do perform all the procedures. I think by tailoring the procedure to the patient one can increase the success rate for their patients. Complications can arise based on the circumstance, no procedure is foolproof.

TPLO procedure
ACL Injuries in Dogs – Diagnosis
Typically a diagnosis of an ACL tear in a dog can be made based on physical exam. The findings of forward movement of the tibia (cranial drawer) generally allows the surgeon to go directly to surgery. Other ways to evaluate the knee are as follows:
Radiographs: Classic radiographic findings are joint swelling, arthritic change and subluxation (forward movement) of the tibia in relation to the femoral. Classic areas of arthritic development are the patella, fabella, tibial plateau and femoral condylar ridges. I recommend the radiograph (x-ray) be taken with the knee and hock in 90 degree flexion. Please note the differences of the normal and affected knee in the radiographs attached. The benefit of radiographs for me is to see mild changes to confirm the diagnosis and to derive my measurements for either the tibial plateau leveling osteotomy (TPLO) or tibial tuberosity advancement (TTA) procedures.
MRI: While this is a very sensitive diagnostic test to run, generally it isn’t performed in veterinary medicine for this issue, unless the more common tests don’t reveal the answer and the patient is still lame. Unfortunately, a MRI will increase costs and not provide a treatment.
Arthroscopy: I am a big proponent of this method. This is performed at the same surgeory as the corrective procedures, prior to them. Fortunately, arthroscopy is a minimally invasive technique of evaluating the joint and gives us the ability to debride (clean-up) the joint. Between 30-50% of dogs will also injure the medial (inside) meniscus and arthroscopy will allow us to address that issue too. This is far less invasive than an open arthrotomy (opening the joint), which is the mainstay of treatment. Also, immediate recovery is a little quicker to, due to the increased nerve endings present in the joint capsule and muscle disruption.
Open Arthrotomy: This is performed by making a large incision into the joint and moving over the patella (knee cap) to visualize the ACL ligament and menisci. While this is the mainstay approach it is the most aggressive. This allows the surgeon to address the ACL and any meniscal tears.
As you have probably noticed, I am biased towards the knee arthroscopy to evaluate the joint as this is the most minimally invasive approach and allow excellent evaluation of the important structures of the joint. When one is proficient at this approach there really is not an increase in surgery/anesthesia time, making it safe and effective.

X-ray of stifle with a ruptured ACL
ACL injuries in Dogs – signs
Many people who I see will ask me what are signs to look for when it comes to knee injuries in dogs. We will go over both signs you may see at home and then describe a common physical exam of a dog with an ACL rupture.
The most common sign an owner will notice is lameness (limping on a particular hind leg).this can vary from holding the leg up and not bearing weight to a mild shifting of weight off of the affected leg during weight bearing. Also, this can be a chronic lameness or an acute limping. It is widely accepted that ACL tears in the larger dog are typically chronic in nature versus traumatic as they occur in humans. This being said, about 30-50% of will rupture the opposite hind leg within their lifetime in comparison to <5% in humans.
Typically the lameness that is noted is a waxing/waning lameness, meaning that there are periods of improvement and then regression. Other signs involve sitting with the limb out from the body and somewhat extended. Muscle atrophy will also occur in dogs with chronic lameness. This mass will return once the knee joint is stabilized.
When you visit a veterinarian, they will be looking at all of the above factors. The most convincing clinical signs are as follows: joint effusion (swelling), pain on hyper extension of the knee, and instability of the joint (termed cranial drawer and tibial thrust). The instability noted is very diagnostic when it comes to ACL tears.
ACL injuries in dogs
ACL injuries are the most common orthopedic injuries seen in the dog. You may also here them referred to as a cranial cruciate ligament rupture (this is the anatomically correct description, but we will call it the ACL since most are familiar with this). When I talk to owners, I try to reference it to what people experience to make it a little easier to understand.
The ACL, while small, is a very major player in stability of the knee. If this is ruptured (partial or complete) this will cause instability to a varying degree which will cause inflammation, arthritis and cartilage wear in the knee.
There are three big forces that the ACL counteracts: knee hyperextension, tibial(shin bone) internal rotation (twisting inward) and cranial (anterior) shear force. When you think about how we rupture our ACL it is usually by hyperextending the knee and a large force (like a linebacker) impacting the knee or by planting your foot and turning abruptly (internal rotation). Most of the time we rupture our ACL by strenuous activity. The third force (cranial shear force) is greater in the dog than you or I. With us, the top of our tibial (tibial plateau) is relatively flat with only a very small angle of inclination. When the top of our tibial meets the rounded femur (thigh bone) there is very little push forward. In the dog, due to the way the dog stands (4 legs) and develops (much higher angle of inclination of the tibia (normally between 20-40 degrees) this push forward is much greater as the tibia meets the femur. Think of a wheel on a hill model – the steeper the hill the more the wheel will roll down it (the hill is the tibial and the wheel is the femur). The ACL runs from the front part of the tibia to the back of the femur and counteracts the above force. When it is torn there is no holding the tibial back as the dog steps and walks on the injured dog.
So this is a little about what a ruptured ACL is, next we will talk about the signs. Have a great Monday and be sure to check back!!!

X-ray of a normal knee
Please look like at the following video: arthroscopic evaluation of the canine stifle joint.
